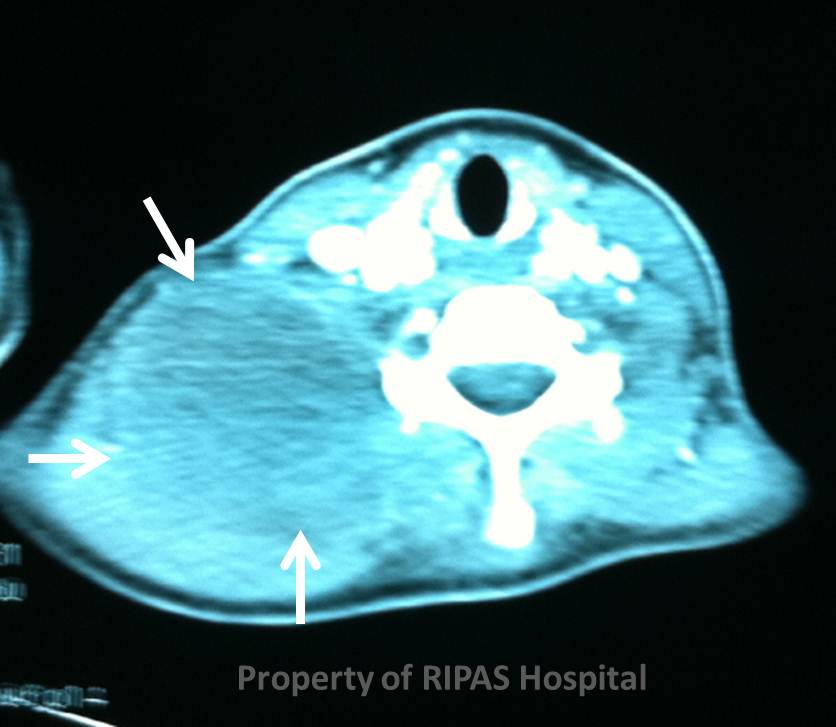
Figure 1: CT Scan of cystic hygroma of the neck (Click on picture to enlarge)
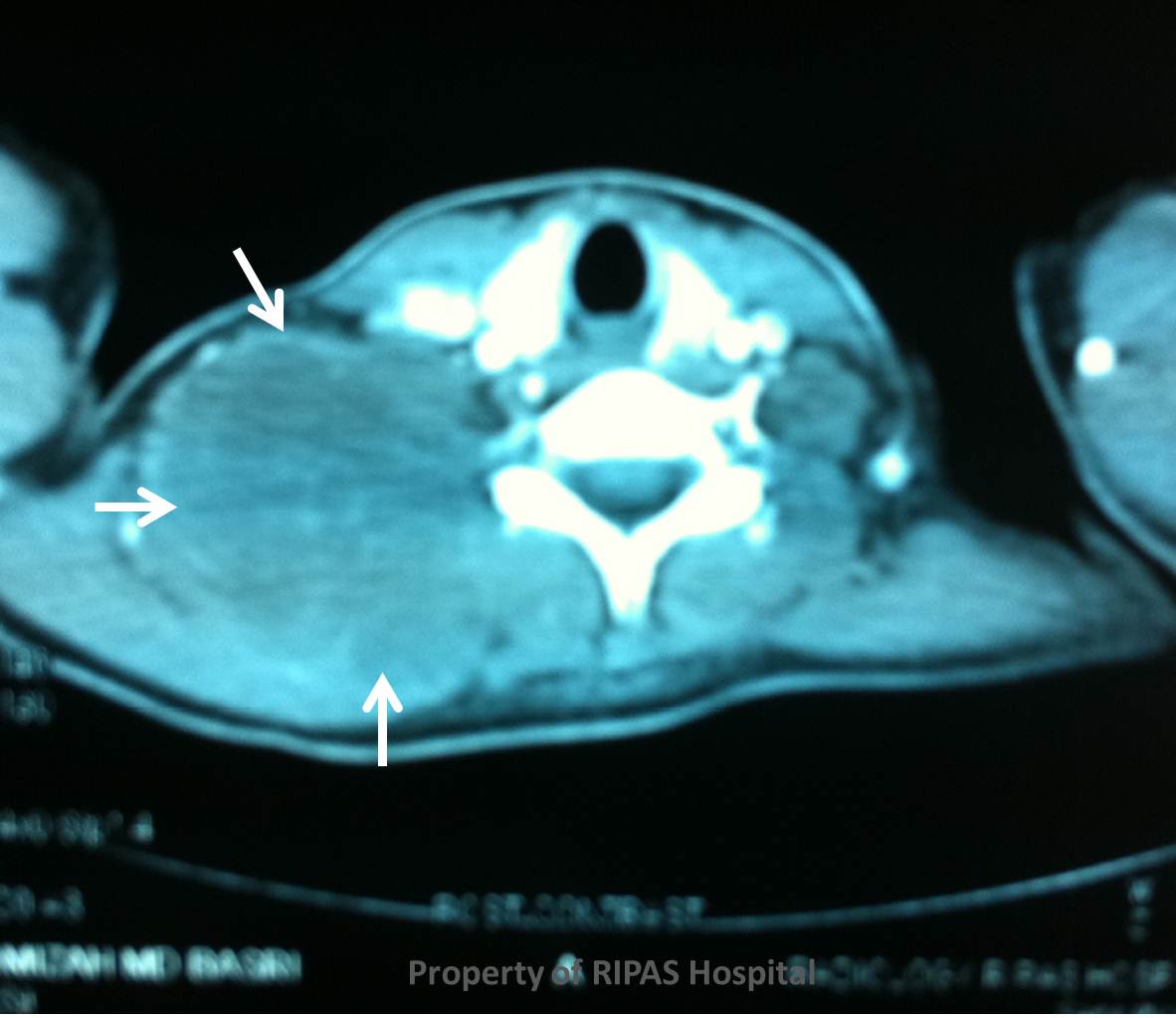
IMAGE OF THE WEEK 2012
WEEK 16
CYSTIC HYGROMA - RADIOLOGICAL APPEARANCE
|
|
Figure 1: CT Scan of cystic hygroma of the neck (Click on picture to enlarge) |
|
|
|
Figure 2: CT Scan of cystic hygroma of the neck (Click on picture to enlarge) |
Imaging is the best modality for investigating cystic hygroma with ultrasound being the first line modality as it is non-invasive and less costly compared with other imaging modality. On ultrasound, cystic hygroma appears typically as large cystic lymphatic spaces which communicates with each other to form larger spaces that infiltrates into surrounding tissues. Extension into the thoracic mediastinum can also be assess using ultrasound although this is limited up to the superior mediastinum.
CT scan is another
useful modality although it incurs significant ionizing radiation. As shown in
the above figures (1 and 2), the lesion is shown as cystic structures that
blends in with the surrounding tissue. In the above case, the sudden increased
in size was the result of bleeding into the cystic hygroma following a fall onto
the right side of the neck.
MRI can provide a high degree of confidence in the diagnosis of cystic hygroma and will further delinate the cystic lesion better particularly the relationship of the lesion to underlying structure and are particularly useful in mediastinal CHs, for which ultrasound is not suitable. With T1 weighted sequences, cystic hygroma presents as a lesion with low signal intensity. On T2 weighted sequences, the lesion appears with a high signal intensity with low signal septation of variable thickness. With good quality MRI images, further imaging modalities are usually not required. False positive MRI scan particularly of haemangiomas can be easily mistaken for cystic hygroma, although the former are more likely to occur in regions not typical of cystic hygroma and the administration of contrast can easily delineate the feeding vessels as well as tumour enhancement to help differentiate haemangiomas from cystic hygromas.
Image and text contributed and prepared by
Mr William Chong, Department of Surgery, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()